
It is widely acknowledged that Australia’s primary health care system is under great strain and is arguably no longer able to meet today’s challenges, including preventing and managing chronic conditions among our communities with diverse needs.
To quote the Federal Health Minister, Mark Butler, the primary health care system is in a “parlous state”. All levels of government, peak medical and allied health professional bodies, primary health networks and research organisations are united in very public calls for urgent reform.
The Government itself, upon its election in May 2022, made reform a priority, and instigated the Strengthening Medicare Taskforce. Following a series of public consultations, the Taskforce has now presented its findings to the Minister for consideration.
Announcements are expected within weeks. These must be accompanied by a strong vision and plan for how we use the public funds available in a different way, to ensure value-based health care can be delivered.
Investments in the primary health sector have not kept pace with changing needs, demands, costs and complexity.
This is not only a result of rebates for GPs falling well behind costs. The matter is one of quality as well as quantity.
As the recent Grattan Institute report into Medicare noted:
“The complexity of GP work has grown immensely, as the population has grown older and rates of mental ill-health and complex chronic disease have climbed. But the model for general practice has changed little. GPs are struggling to fit more and more care into appointments that still average 15 minutes, and lack the support of a broader team.”
This situation, already well embedded, was significantly exacerbated by the onset of the COVID-19 pandemic. The effects have been multiple, and continue to evolve. Three aspects are of especial note within the context of current and future stresses on delivery of primary health care:
- Coronavirus itself, and the stresses of pandemic management, continue to impact demand on health services and staff numbers in the short and long term.
- The emergence of long COVID poses as yet unanswered questions concerning its complexity, persistence and treatment.
- Deferred care for other issues has increased demand and, where conditions have worsened, may require more complex and costly treatments.
A January 2023 survey by non-profit health care comparison service Cleanbill found that across the country just 42.7 per cent of practices bulk bill all patients without levying additional fees. The rest charge some or all patients about $40 extra for a standard consultation – pushing up basic health costs and potentially deterring people from seeking treatment.
Indeed, in January Minister Butler confirmed that in most cases the patient gap fee is now higher than the Medicare rebate.
With all this in mind, it is difficult to disagree with the conclusion of Grattan Institute report authors Peter Breadon and Danielle Romanes that Medicare is “a system designed for an earlier era [which] hasn’t been updated to respond to the rise of chronic disease, or to tackle gaping disparities in access to care, rates of disease, and life expectancy.”
At federal and state levels the appetite for reform is manifest. How that is to be achieved, however, remains to be seen.
It is also important to reduce the waste and inefficiencies wherever possible. In many cases at present, funding is provided to practitioners and accessed by patients in ways that create disincentives to proactive, preventative and planned care, delivered by a team of health professionals that addresses physical, social and emotional wellbeing.
Funding needs to be designed and delivered to drive value, including creating a team approach to integrated care for those with chronic conditions, and ensuring that the patient is an active participant in the process instead of simply a passive recipient.
This requires the health system, and the resources made available to it, to utilise the expertise of all health professionals. Maximising scope to the top of roles, enabling team-based care and looking at new workforce models will be critical.
Further, it is essential that cooperation across all levels of the health care system, and regardless of funding source, work more closely together. Fragmented policy and funding structures embed disincentives that can prioritise provider management over patient outcomes.
We suggest that all decisions on system reform should be guided by improvements against the Quintuple Aim of health care – a widely accepted summation of universal health practice priorities.
The Quintuple Aim holds that any health care system must deliver these outcomes:
- improved population health
- enhanced care experience
- reduced costs
- reduced practitioner burnout through better working conditions
- improved health equity
Critically, the model holds that these outcomes are not in opposition to each other. For example, it is entirely possible to improve patient care without increasing the cost of delivering it.
Organisations such as the Australian Medical Association have called for the Medicare rebate for GP consultations to be doubled. We understand the intention, and will be interested to see if the Taskforce makes such a recommendation or instead suggests more complex range of solutions, in which rebate increases form part of a raft of economic measures.
Another way to improve health equity lies in fixing the imbalance inherent in the way MBS and PBS co-payments are levied.
Recent research shows that out-of-pocket costs to patients are proportionally greater for those on low incomes than they are for the more well off.
This is especially so in the matter of medications covered by the Pharmaceutical Benefit Scheme, for which a co-payment is levied. A paper published late last year in the journal Health Policy looked at the percentage of disposable income used to cover out of pocket MBS and PBS costs.
It found: “Percentages decreased from 1.16 per cent in the poorest decile to 0.63 per cent in the richest decile for MBS costs, and from 1.35 per cent to 0.34 per cent for PBS costs.” PBS cost structures, in particular, the authors concluded, are “distinctly regressive”.
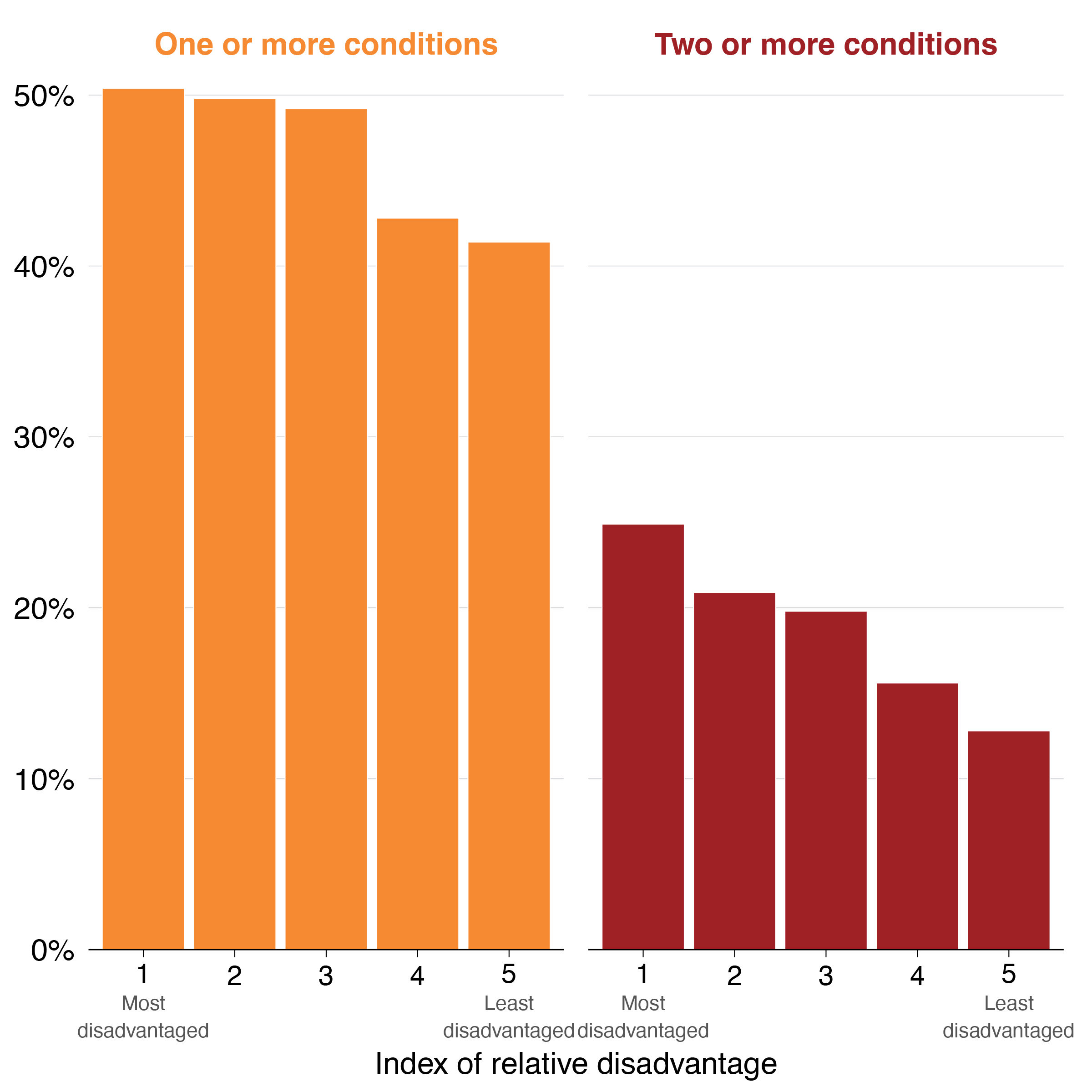
There is an abundance of research – which is reflected in North Western Melbourne Primary Health Network’s latest triennial Health Needs Assessment – that indicates a clear correlation between socioeconomic status and demand for health services at every level. Low incomes – sometimes compounded by factors such as education, cultural and language background, and at-risk status – are directly related to increased need for treatment for chronic physical and mental illness.
The Quintuple Aim implies that co-payments, when levied, should be progressive in structure. Current PBS and MBS costings superficially appear to meet that aim, but in reality the system places the heaviest demands on those with the least capacity to meet them.
If Medicare is to be properly strengthened, it must be adjusted to deliver universal and equitable health care to all. We recognise that this will not be an easy reform to achieve. Neither is it a challenge unique to Australia.
Indeed, in a major paper published in April 2022 The Lancet Global Commission identified weaknesses in primary health care (PHC) as a worldwide and worsening phenomenon.
“Public funding for PHC is insufficient, access to PHC services remains inequitable, and patients often have to pay out of pocket to use them,” the authors wrote.
“A vicious cycle has undermined PHC: underfunded services are unreliable, of poor quality, and not accountable to users. Therefore, many people bypass primary health care facilities to seek out higher-level specialist care. This action deprives PHC of funding, and the lack of resources further exacerbates the problems that have driven patients elsewhere.”
The Australian Government, with a fresh mandate and the Taskforce’s findings to hand, has a once-in-a-generation opportunity to begin to restructure the country’s precious universal health care system in a way that bakes in access and treatment for all for many decades to come.
As well as the work of the Taskforce, the government has at its disposal substantial, and largely harmonious, research and recommendations from sources such as The Grattan Institute and a recent Canberra summit involving delegates from all major health peak bodies.
It is a truism that complex problems are never solved simply by throwing money at them. However, it is also true that underfunded systems cannot be reformed without first providing them with the financial resources they require.
We, along with the entire health sector, look forward to imminent announcements regarding Medicare’s future. We hope that any welcome boost to funding will be accompanied by plans – and the will – to tackle the emergent inequities in the system, and the desire to restore it to the world-class structure it was always intended to be.


