
Health professionals – including GPs and pharmacists – should stop directing asthma patients to use as-needed short-acting beta2 agonists (SABA) alone to manage their condition.
That’s the updated advice from the latest edition of the National Asthma Council’s Australian Asthma Handbook.
The advice applies to people aged 12 and over who have asthma. It also has implications for people at risk of thunderstorm asthma.
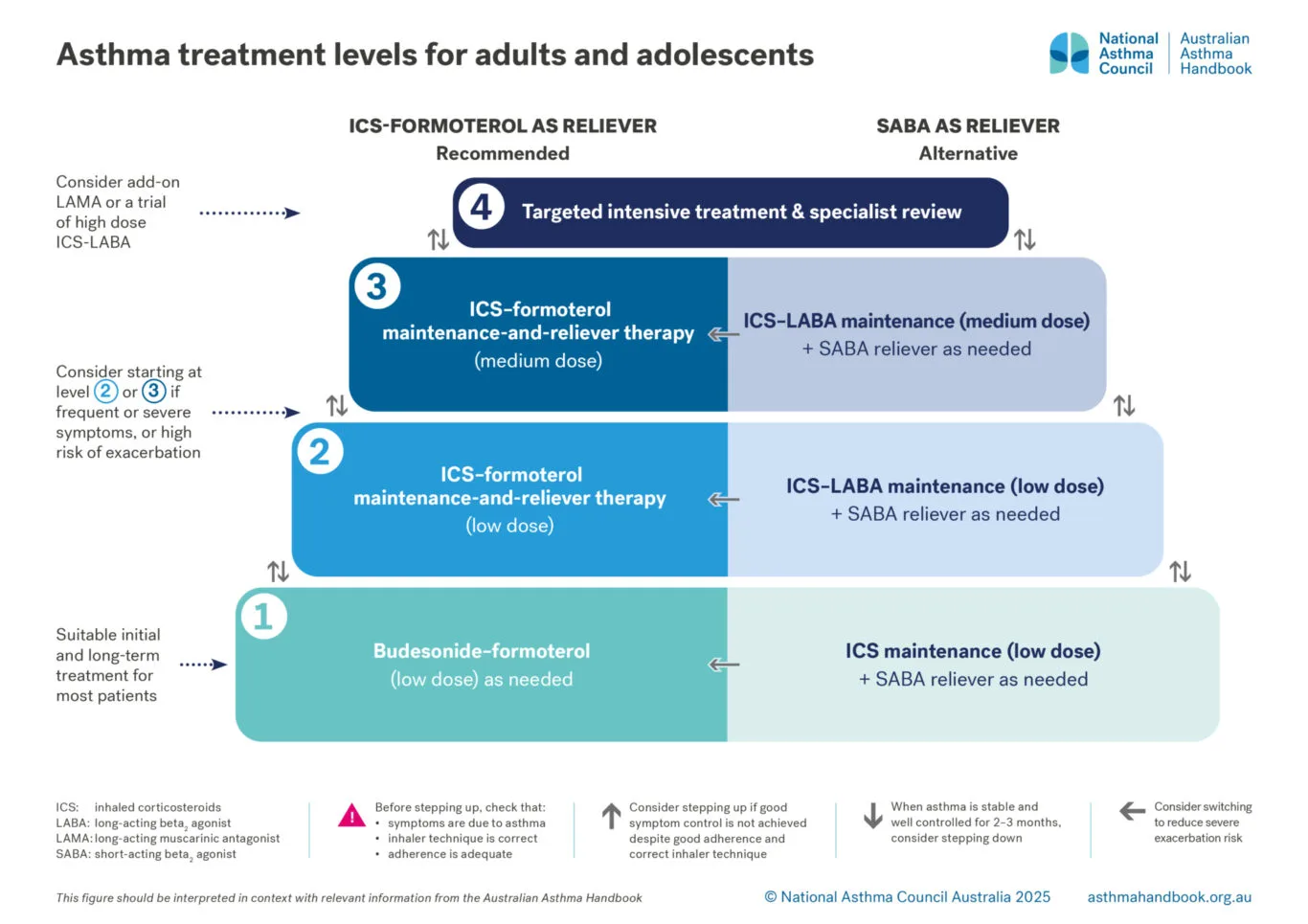
Instead of as-needed SABA, the handbook now recommends either anti-inflammatory reliever (AIR) therapy, or maintenance-and-reliever therapy (MART).
All people aged 12 or over who have asthma need inhaled corticosteroid therapy (ICS).
Why the change?
Several studies cited in the Handbook collectively establish that as-needed SABA alone, even for the relief of mild asthma, is linked to a greater likelihood of severe flare-ups. In contrast, using AIR therapy or maintenance treatment with a low-dose ICS significantly lowers this risk.
“The common approach was starting patients with mild asthma on SABA as-needed – however, this did not treat the underlying inflammation,” says Professor Nick Zwar, chair of the National Asthma Council’s guidelines committee.
“Starting patients on the new recommendation for low-dose budesonide-formoterol as needed offers a more evidence-based approach to asthma management and reflects the biology of the condition.”
For those not using a regular ICS, taking low-dose budesonide-formoterol only when symptoms arise has been shown to significantly lower the risk of severe asthma flare-ups that require oral corticosteroids, compared to using SABA alone.
The new handbook has some clear escalation charts for managing asthma in adolescents and adults.
It also renews advice that all asthma patients need to have a written asthma action plan, provided by a GP.
This includes directions for patients in the event of worsening symptoms. It should be reviewed regularly. Pharmacists are advised to discuss asthma action plans with customers who request either a script-authorised or over-the-counter SABA inhaler – and to refer them to their GP if the plan is outdated or a change in symptoms is reported.
Thunderstorm asthma
In people with allergy to grass pollens – with or without known asthma – thunderstorm asthma can be triggered by exposure to a high concentration of pollen fragments in wind gusts at the start of a thunderstorm.
In Victoria, this mainly occurs in springtime or early summer, and is associated with high perennial rye grass pollen counts.
Research shows that people with pollen allergies, but without known asthma, who self-manage their risk by using only an over-the-counter SABA inhaler are at high risk of severe exacerbations during thunderstorms.
New advice says people in this cohort should also use an ICS inhaler, which appears to be protective.
People with asthma and known grass pollen allergy or springtime allergic rhinitis should receive ICS treatment and advice on avoidance during pollen season: on days when there is a high concentration of ryegrass pollen in the air and thunderstorms are predicted, they should avoid exposure outdoor air, especially gusty winds before the rain.
All patients at risk of thunderstorm asthma, regardless of asthma status, should:
- receive individually optimised ICS-containing treatment
- make sure their reliever is in date and contains an adequate number of doses throughout the pollen season in their region.
For detailed information on symptoms and managing risk, see this NWMPHN webpage.
For more information:
- Australian Asthma Handbook | National Asthma Council
- Australian Asthma Handbook – what’s new | National Asthma Council
- Asthma in Adolescents (Aged 12 Years and Over) | HealthPathways Melbourne


